Background: Due to the pandemic outbreak, healthcare providers are at a higher risk of contracting COVID-19 than the general population. In addition to practicing and following 6′ distancing guidelines, which is not always possible given the various tasks and limited space, face shields have become a critical piece of personal protective equipment to decrease the spread of COVID-19.
Study Description: In partnership with Virginia Tech, a generative study was conducted to develop design criteria for current face shield improvements as well as to better understand the usability of the current existing face shield, and whether it improves or hinders healthcare providers’ work.
Thereafter, a multi-phase iterative qualitative usability study was conducted with clinicians and healthcare workers to evaluate the usability of the features developed and iteratively improve the design with feedback. A total of three phases of face shield prototypes were developed, each phase addressed the reported issue from its former.

Phase 1 started with a survey to capture the current existing face shield design issues. A total of six different face shield designs were found. These designs were chosen because they were immediately available to Healthcare Personnel through dissemination from the materials management team at a single healthcare institution. Participants were asked to provide feedback on the most frequently used face shield type. The survey consisted of four questions, three of which were quantitative questions, one was an open-ended free text response.

Phase 2 design was prototyped by Terrestrial Robotics Engineering and Controls Lab (TREC) at Virginia Polytechnic Institute and State University (Virginia Tech). This design contains two components: (1) headband (inner piece), (2) articulating arm (outer piece). The two-component face shield design provides the following three features: (1) three holes on each side of the headband which allow users to choose the preferable distance between face shield to face, (2) the feature of flipping the face shield up and down is enabled with the connection of two components, and (3) attachable elastic straps from ear to ear.

Phase 3 similar to phase 2 design, an additional built-in hat bill was added on the headband to further prevent aerosol droplets entering from the top.
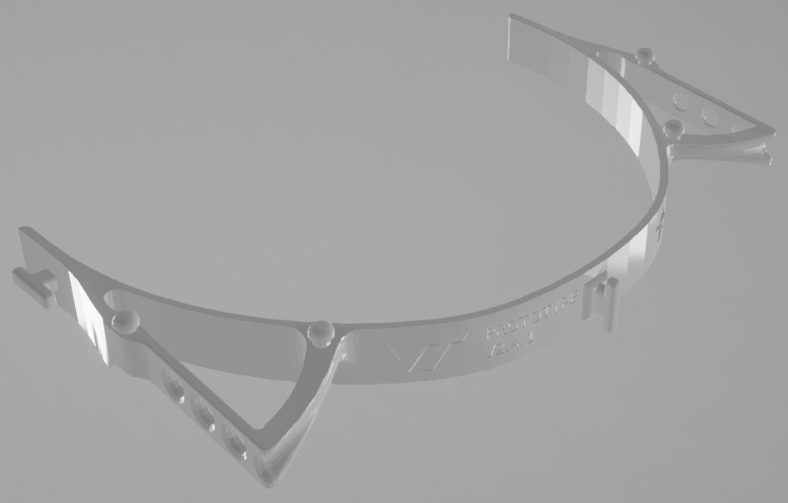
Phase 4 given the increased tightness and inflexibility from phase 3’s headband (built-in hat bill), the issue of headache was largely reported. To address this, in phase 4 the built-in hat bill was removed, and four pegs were added on the top of headband (two on each side), provided attachable connections for opaque plastic.